Rotator Cuff Injury
The most common shoulder joint condition, which can occur as early as middle age. The shoulder/arm bone is held in place by four muscles (rotator cuff), attached to the shoulder blade and chest. This loose, muscular connection allows for extensive shoulder movement. Above the rotator cuff lies the protrusion of the shoulder blade (acromion), with a bursa between them providing smooth sliding. If the shoulder is not in the ideal position, or due to chronic overuse, the arm bone and roof (acromion) trap one of the tendons of the rotator cuff (supraspinatus), causing shoulder pain, bursa inflammation, and eventually tendon injury. In severe cases, the tendon may tear, further compromising shoulder biomechanics, and eventually damaging other tendons. Of course, accident or certain sports injuries can alter this otherwise typical sequence of injuries.
Treatment
The initial treatment always involves physical therapy, manual therapy, aiming to restore ideal biomechanics. Among minimally invasive methods, PRP treatment aims to heal damaged tissues. It is recommended for early and moderately severe conditions, and its long-term results are clearly better than steroid injections1. Healing with PRP may take 2-3 months. The effect of steroids is usually immediate, however, the effect of repeated steroid injections diminishes, and joint steroid contributes to the progression of arthritis (wear and tear)2. In severe cases, surgery may provide relief.
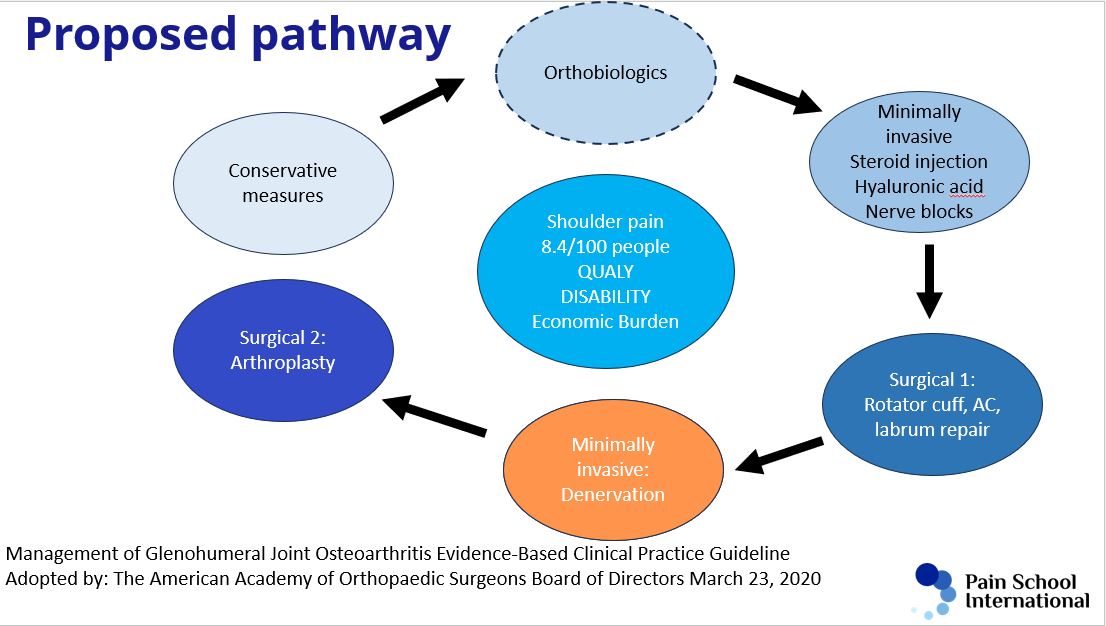
Shoulder wear and tear (arthritis/osteoarthritis)
The second most common type of shoulder joint condition is arthritis/wear and tear/arthrosis, which occurs as a result of overuse or aging. It usually affects those over 50 years old. The cartilage of the shoulder joint thins, the joint becomes painful, and the range of motion decreases. In addition to constant dull pain, stabbing pain usually occurs with bad movements.
Treatment
It is always advisable to try physical therapy, manual therapy. If ineffective, minimally invasive solutions come into play. Regenerative therapy may be beneficial in not very advanced cases, but its success is questionable in severe cases. Steroids can be tried, but it should always be remembered that despite its miraculous short-term effect, long-term use of steroids deteriorates the condition of the cartilage(2). Denervation of the shoulder joint (elimination of innervation) can bring relief in cases where surgery is not recommended for the patient. The technique, used in many countries around the world, was developed by Dr. Ágnes Stogicza3. Currently, a clinical trial is underway at our Pain Clinic in collaboration with the University of Toronto and the Albert Einstein University of Sao Paulo to measure the effectiveness of the intervention. I am participating in the trial.
AC Joint Wear, Instability
The AC (acromioclavicular, collarbone-shoulder blade) joint is located between the collarbone and the protrusion of the shoulder blade, forming the roof above the head of the humerus in the shoulder joint (Video 4 shoulder).
Instability may develop, in which case the joint connecting the collarbone and the protrusion of the shoulder blade widens, compromising shoulder joint biomechanics.
Treatment
It responds particularly well to regenerative treatment, which not only reduces pain but also increases shoulder joint stability. Steroid injections alleviate the symptoms often temporarily, but do not affect the instability.
Source:
1. de Sanctis EG, Franceschetti E, De Dona F, Palumbo A, Paciotti M, Franceschi F. The efficacy of injections for partial rotator cuff tears: A systematic review. J Clin Med. 2021;10(1):1–15.
2. McAlindon TE, LaValley MP, Harvey WF, Price LL, Driban JB, Zhang M, et al. Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis a randomized clinical trial. JAMA – J Am Med Assoc. 2017;
3. Stogicza AR, Peng P. Cryoanalgesia for shoulder pain: a motor-sparing approach to rotator cuff disease. Reg Anesth Pain Med. 2022;47(9):576–80.