What are Cervicogenic Headaches?
This very common type of headache (20–30%) is caused by disorders of the cervical spine. These include cervical disc herniation, degeneration of the cervical facet joints, tension in the neck muscles, and irritation of the upper spinal nerve roots.
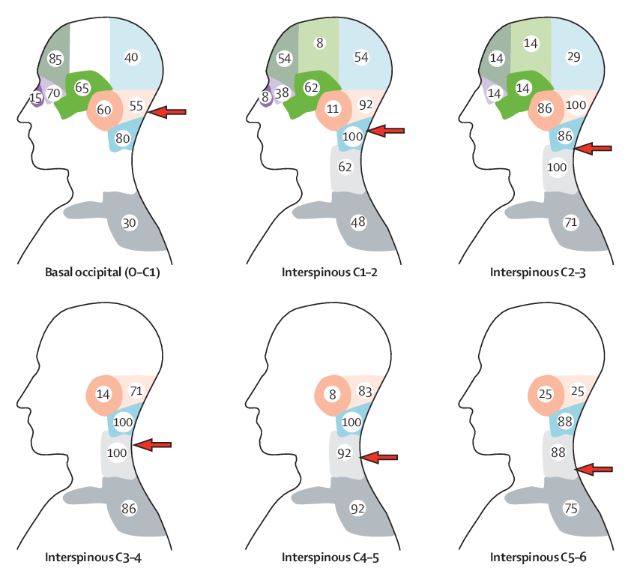
The pain typically starts in the occipital region and radiates to the top of the head and behind the eyes. It can be unilateral and may even spread from one side to the other. Pain originating from the cervical facet joints may radiate to the neck, head, and vertex¹.
Typical patients are those who have suffered trauma and whiplash injury (Whiplash Associated Disorder (WAD)) (car accidents, snowboarding, cycling accidents, etc.), and another large group includes those with chronic postural disorders (e.g. dentists, people working at a computer), as well as individuals with genetically weaker connective tissue.
To clarify the diagnosis, the patient’s medical history, physical examination, and imaging studies are required (cervical MRI, flexion-extension X-ray, DMX (Digital Motion X-ray)).
Treatment
Their treatment is multi-faceted, including lifestyle changes, posture improvement, physical therapy, manual therapy, and minimally invasive approaches such as stem cell or PRP treatment for facet joints and discs, which can regenerate neck ligaments, improve neck mechanics, and potentially prevent or slow down degenerative processes.
PICL
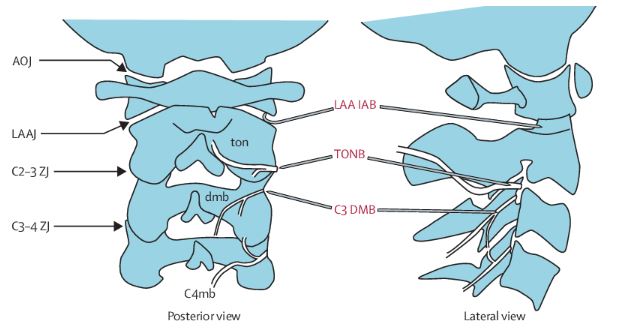
With PICL (Percutaneous Implant of Craniocervical Ligaments) treatment, regenerative therapy of the head–neck junction is possible. During the procedure, stem cells or PRP are injected under X-ray guidance into the atlantoaxial (central and lateral) and atlanto-occipital joints, as well as the functionally related ligaments.
In such cases, the lower segments of the cervical spine are usually treated as well.
Usually, the lower part of the cervical spine is also treated.
Further treatment option is cervical medial branch radiofrequency ablation. During this procedure, the nerve supply of the cervical facet joints is interrupted, thereby reducing pain sensation².
This procedure is always preceded by a diagnostic injection.
Source:
1. Bogduk N, Govind J. Cervicogenic headache: an assessment of the evidence on clinical diagnosis, invasive tests, and treatment. Lancet Neurol [Internet]. 2009;8(10):959–68.
2. Manchikanti L. Facet joint pain and the role of neural blockade in its management. Curr Rev Pain. 1999;3(5):348–58.